 HANDS OFF! would be a welcome policy for hospitals to implement. Unfortunately I cannot see this happening any time soon, especially in private hospitals. The frequent ‘diagnosis’ of an ‘anterior lip’ in labour causes much alarm among the staff, which then transfers to the labouring woman. An anterior lip simply means there is some cervix still present or as is often diagnosed – ‘swelling of the cervix’, prior to full dilation.
HANDS OFF! would be a welcome policy for hospitals to implement. Unfortunately I cannot see this happening any time soon, especially in private hospitals. The frequent ‘diagnosis’ of an ‘anterior lip’ in labour causes much alarm among the staff, which then transfers to the labouring woman. An anterior lip simply means there is some cervix still present or as is often diagnosed – ‘swelling of the cervix’, prior to full dilation.
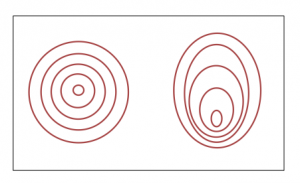
At some point in labour most women will have an anterior lip because this is the last part of the cervix to be pulled up over the baby’s head. The cervix does not open in a nice neat circle. It depends on the position of the baby. If a baby is in the most favourable position, i.e. anterior (OA), then the cervix is more likely to open evenly, but if baby is in a posterior position (OP) or somewhere inbetween, then the opening of the cervix will be uneven.
A woman in a private hospital, who was planning a normal, non-interventionist birth, had been in labour for about 10hrs. and was 9cms dilated. Private hospital midwife (obstetric nurse!) was following instructions and did a ‘routine’ vaginal examination only to discover an anterior lip. Panic stations ensued and the obstetrician was called. On arrival he, of course, did another vaginal examination, announcing that she was only 8cms., swollen cervix, swelling on baby’s head, meconium in waters and she could stay like that for hours OR he had 1 free operating theatre available – right now – and she could be holding her baby within the hour! Overwhelmingly powerful suggestion!
She had the caesarean section and was separated from her baby, due to the hospital policy of baby needing to be monitored following a caesarean.
If she could do this birth again, in a different environment, with different caregivers, and no vaginal examinations, the outcome may well have been very different. As a doula we need to discuss with women about vaginal examinations. The information from a vaginal examination, is irrelevant, except in a few extreme circumstances. We need to give women time to follow their body’s lead, to be in tune and trust their birthing instincts, allowing time for labour and birth to ‘happen’, as it should, without time frames and judgements.


{kind=link}
{kind=link}
{kind=link}
{kind=link}